Effect of Age-Related Hearing Loss on Neuropsychological Test Performance
Wong, Christina G. PhD; Rapport, Lisa J. PhD; Stach, Brad A. PhD; Ramachandran, Virginia AuD, PhD
Interest is growing in the association of hearing loss with other health conditions, especially cognitive disorders such as dementia. In addition, health care providers in general are being asked to routinely screen patients for common problems associated with aging, including cognitive impairment. But can hearing loss invalidate these measures? If the measures that are used to assess these problems are unduly influenced by hearing loss, they might be misinterpreted in those who do not hear well. In other words, could patients be misdiagnosed or inaccurately identified as having cognitive impairment because of hearing loss alone? We sought to answer this question by addressing the effect of hearing loss on a battery of neuropsychological measures.
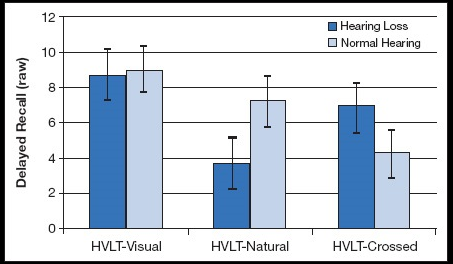
(see Figure 1)
HVLT-R Delayed Recall raw scores for the hearing loss group (n = 41) and normal hearing group (n = 41) by presentation condition. Mixed-model ANOVA indicated that there were significant main effect of condition and significant group by condition interaction with large effect sizes, F(2, 79) = 27.56, p <.001, ηp 2 =.41. Hearing loss, cognition, dementia. (Source: Effect of Age-Related Hearing Loss on Neuropsychological Test Performance. The Hearing Journal73(3):16,17, March 2020.)
{kind=link}
Neuropsychological assessment involves the administration of standardized cognitive tests to examine how an individual performs in areas such as memory, language, and other thinking abilities. These evaluations are often used to identify cognitive impairments that may indicate the presence of a neurocognitive disorder such as dementia. Many cognitive tests, particularly in the area of verbal memory, require the examinee to learn and remember information that is presented orally.1 Therefore, individuals with hearing loss may be at a disadvantage to perform optimally on verbal memory tests. Difficulty with accurately hearing the information provided or expending extra cognitive effort to listening may suppress an individual’s memory test scores, putting them at risk of being over diagnosed with cognitive impairment.2 Our study aimed to determine the effect of age-related hearing loss on verbal memory performance in older adults.3
STUDY HIGHLIGHTS
We recruited 41 adults with mild-to-severe sensorineural hearing loss (average PTA = 49.2 dB HL, SD = 12.9) and 41 adults with hearing in the normal range (average PTA thresholds < 25 dB HL). Participants ranged in age from 55-80 years old (average age = 66.7 years, SD = 6.5), and were free of dementia or other neurologic/psychiatric conditions that could interfere with cognitive testing. Because age is strongly related to hearing loss, the groups were matched on age (± 3 years) and did not differ in terms of gender proportion.
For the study, both groups completed a commonly used verbal memory test called the Hopkins Verbal Learning Test–Revised Edition (HVLT-R).4 This test involves learning a list of words over repeated presentation trials and recalling the words after a 20- to 25-minute delay. The test was given in a standard auditory format, in which participants wore noise-cancelling headphones and viewed video recordings of an examiner presenting the test. Hearing loss participants did not wear their hearing aids during the auditory version because of difficulties related to controlling for differences in hearing aids and because some participants with hearing loss did not have hearing aids. We thought this decision was ecologically valid because patients frequently attend clinical neuropsychological assessment appointments without their hearing aids or without ever having pursued treatment.5 Moreover, the majority of adults with hearing loss do not wear hearing aids due to several barriers, including cost and stigma.6 For the auditory presentations of the HVLT-R, we presented the tests to the two groups under two conditions: In the natural auditory condition, both groups heard the test at a normal speaking volume. In the crossed auditory condition, adults with hearing in the normal hearing range were presented the HVLT-R video with simulated hearing loss, in which the audio was edited to mimic age-related hearing loss (i.e., proportionately greater loss in high frequencies of >1 kHz compared with lower frequencies, 0.25 to 1 kHz). Adults with hearing loss were afforded amplified acoustic intensity for the crossed condition. Lastly, the test was also administered to each participant in an experimental visual format for which the word list was presented as printed words on a computer screen; this version did not include an auditory component.
Results for the delayed recall trial under the different presentation conditions are displayed in Figure 1. We found that participants with hearing loss performed significantly worse on the natural auditory verbal format compared with participants without hearing loss. They learned fewer words during the presentation trials and recalled fewer words after a delay. Interestingly, the results also demonstrated that, although hearing loss participants learned fewer words, they generally remembered the words that they did learn after the delay. This finding suggests that participants with hearing loss did not have a deficit in storing the information in memory, which is a characteristic of amnestic disorders such as mild cognitive impairment and dementia due to Alzheimer’s disease. When performance on the visual version of the memory test was examined, we found that the performance of the hearing loss group was equivalent to that of the group without hearing loss, and effect sizes of any differences were small and not statistically significant. Lastly, for the crossed auditory condition, the group without hearing loss performed significantly worse than the hearing loss group. The groups did not differ in neuropsychological measures of attention, processing speed, executive function, or figural memory.
CLINICAL IMPLICATIONS
As expected, unaided hearing loss adversely affected performance on a verbal memory test when it was presented in the conventional auditory format at a normal speaking volume. In contrast, older adults with hearing loss had equivalent performance to those without hearing loss on a novel visual version of the memory test. Moreover, although they performed well under natural conditions, adults without hearing impairment who experienced simulated hearing loss performed as poorly as adults with hearing loss. These findings indicate that the standard auditory format may overestimate cognitive impairment in older adults with hearing loss, and an alternative visual version of the test may improve validity of verbal memory assessment in this population.
The association between hearing loss and dementia is potentially inflated because of the high reliance on auditory-verbal memory tests to diagnose dementia. Our findings demonstrate that individuals with hearing loss can falsely appear impaired on these measures. A body of literature has reported an association between hearing loss and increased risk for cognitive impairment and dementia.7 The underlying mechanisms for this relationship remain unclear;8 however, studies that do not account for the contribution of hearing loss to auditory cognitive test performance inflate the strength of the association. On an individual patient level, it is important that clinicians are especially mindful of the effects hearing loss can have on cognitive measures that involve auditory stimuli to avoid false-positive diagnoses of cognitive disorders. Our findings are consistent with those in other research that has demonstrated that reduced audibility results in impaired performance on verbal memory tests and cognitive screeners.2,9
Overall, this study indicates that auditory-verbal memory performance should be interpreted with caution in individuals with hearing loss. Future research should examine the effect of hearing aid use on auditory-verbal memory tests commonly used in clinical and research contexts. For individuals with severe-to-profound hearing loss in whom the use of hearing aids or other amplification is not sufficient, visual versions of verbal memory assessments should be validated for clinical use to facilitate comprehensive neuropsychological assessment rather than omitting tests with an auditory component. Interdisciplinary collaboration between audiologists and neuropsychologists will improve our understanding of the complex relationship between hearing loss and cognition, and lead to important implications for the clinical care of patients with hearing loss.
*This research was funded by a grant from Blue Cross Blue Shield of Michigan.
REFERENCES
9. Jorgensen LE, Palmer CV, Pratt S, Erickson KI, Moncrieff D. The effect of decreased audibility on MMSE performance: A measure commonly used for diagnosing dementia. J Am Acad Audiol. 2016;27(4):311-323.