Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Synopsis of the 2017 American College of Cardiology/American Heart Association Hypertension Guideline
Robert M. Carey, MD; Paul K. Whelton, MB, MD, MSc; for the 2017 ACC/AHA Hypertension Guideline Writing Committee
March 6, 2018 (Annals of Internal Medicine)
Abstract
Description: In November 2017, the American College of Cardiology (ACC) and the American Heart Association (AHA) released a clinical practice guideline for the prevention, detection, evaluation, and treatment of high blood pressure (BP) in adults. This article summarizes the major recommendations.
Methods: In 2014, the ACC and the AHA appointed a multidisciplinary committee to update previous reports of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The committee reviewed literature and commissioned systematic reviews and meta-analyses on out-of-office BP monitoring, the optimal target for BP lowering, the comparative benefits and harms of different classes of antihypertensive agents, and the comparative benefits and harms of initiating therapy with a single antihypertensive agent or a combination of 2 agents.
Recommendations: This article summarizes key recommendations in the following areas: BP classification, BP measurement, screening for secondary hypertension, nonpharmacologic therapy, BP thresholds and cardiac risk estimation to guide drug treatment, treatment goals (general and for patients with diabetes mellitus, chronic kidney disease, and advanced age), choice of initial drug therapy, resistant hypertension, and strategies to improve hypertension control.
Hypertension is the leading cause of death and disability-adjusted life-years worldwide (1, 2). In the United States, hypertension accounts for more cardiovascular disease (CVD) deaths than any other modifiable risk factor and is second only to cigarette smoking as a preventable cause of death for any reason (3). The 2017 American College of Cardiology (ACC)/American Heart Association (AHA) Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults provides an evidence-based approach to reduction of CVD risk through lowering of blood pressure (BP) (4).
Guideline Development Process
In 1977, the National Heart, Lung, and Blood Institute (NHLBI) initiated a series of hypertension guidelines, culminating in the 2003 publication of The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) (5). In 2013, the NHLBI transferred responsibility for sponsorship of clinical practice guidelines for CVD prevention to the ACC and the AHA (6). In 2014, the ACC and the AHA partnered with 9 other professional associations to develop a new hypertension clinical practice guideline. A 21-member panel of multidisciplinary experts (physicians, nurses, pharmacists, and patient representatives) with no BP-related industry relationships developed the 2017 guideline.
The writing committee conducted a structured review of the literature and commissioned 4 systematic reviews (and meta-analyses when feasible) from an independent evidence review committee to address the following: 1) self-directed and/or ambulatory BP monitoring compared with office-based BP measurement to prevent adverse outcomes and achieve better BP control, 2) the optimal target for BP lowering during antihypertensive therapy, 3) whether various antihypertensive drug classes differ in their comparative benefits and/or harms as first-line treatment, and 4) whether initiating treatment with 1 antihypertensive drug (monotherapy) is more or less beneficial than starting with 2 drugs (7).
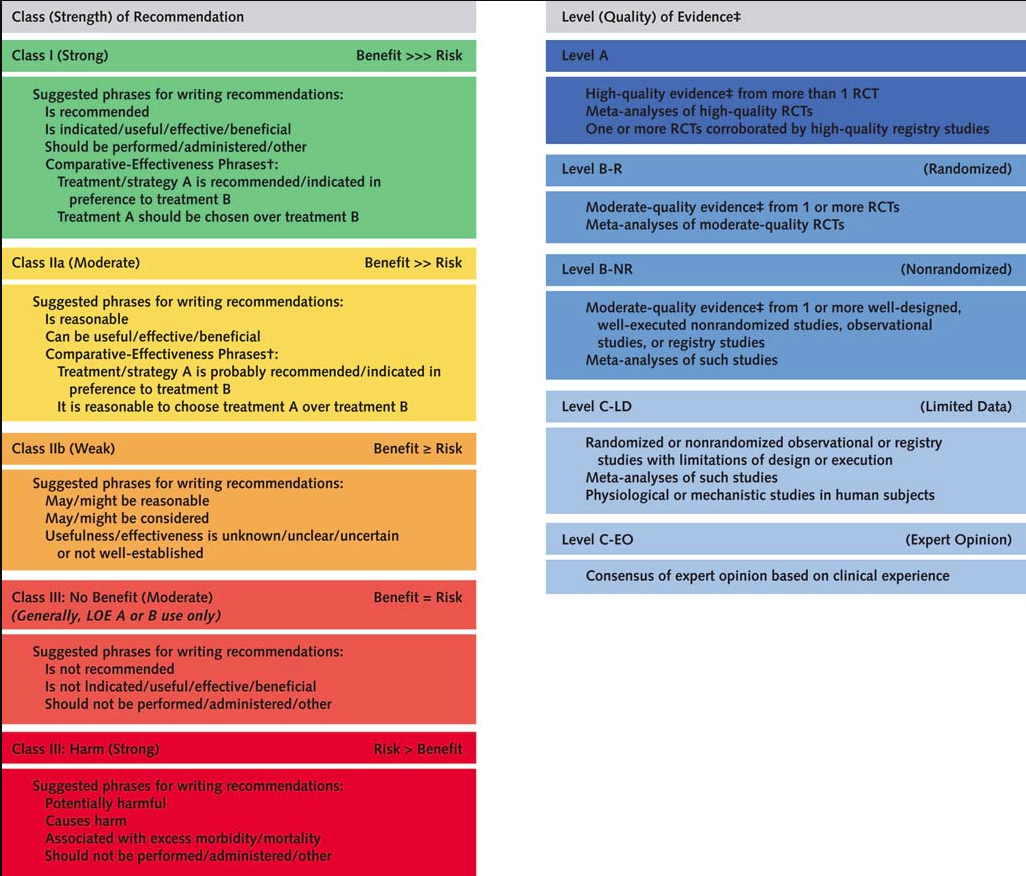
The writing committee used the methods of the ACC/AHA Task Force on Clinical Practice Guidelines (8) to make 106 recommendations, each characterized by class (strength) of recommendation (an estimate of the magnitude and certainty of benefit in proportion to risk) and level (quality) of evidence (rating the type, quantity, and consistency of data from clinical trials and other sources). Five “official” reviewers from the ACC and the AHA, 9 “organizational” reviewers representing the partner professional organizations, and 38 “content” reviewers with expertise in hypertension reviewed the recommendations before approval by the governing bodies of the ACC, the AHA, the American Society for Preventive Cardiology, the Preventive Cardiovascular Nurses Association, the American Academy of Physician Assistants, the Association of Black Cardiologists, the American Pharmacists Association, the American College of Preventive Medicine, the American Society of Hypertension, the American Geriatrics Society, and the National Medical Association. A complete description of the methods, the evidence reviews, and the recommendations is available at www.acc.org/latest-in-cardiology/ten-points-to-remember/2017/11/09/11/41/2017-guideline-for-high-blood-pressure-in-adults. This synopsis summarizes major recommendations for generalist clinicians.
Recommendations
Classification of BP and Diagnosis of Hypertension
Table 1 shows BP classifications. Although the definition of normal BP remains the same as in JNC 7 (average systolic BP [SBP] <120 mm Hg and average diastolic BP [DBP] <80 mm Hg), the 2017 guideline replaces the term “prehypertension” with “elevated BP” (average SBP of 120 to 129 mm Hg and average DBP <80 mm Hg) and “stage 1 hypertension” (average SBP of 130 to 139 mm Hg or average DBP of 80 to 89 mm Hg). Stage 2 hypertension is defined as an average SBP of at least 140 mm Hg or an average DBP of at least 90 mm Hg instead of a BP of at least 160/100 mm Hg. The upper end of prehypertension was reclassified as stage 1 hypertension because adults with BP in this range have an approximately 2-fold increase in CVD risk compared with adults with normal BP, and recent randomized clinical trials have demonstrated benefit with an SBP below 130 mm Hg (9–13). This change in BP classification is estimated to result in an increase of about 14% in the prevalence of hypertension in the United States but only a 1.9% increase in adults requiring antihypertensive drug therapy (14).
Measurement of BP
Proper methods of BP measurement, which are detailed in the guideline (4), are fundamental to categorizing BP, ascertaining BP-related CVD risk, and managing hypertension. The guideline urges clinicians to obtain accurate measurements and base their estimates of BP on an average of at least 2 readings obtained on at least 2 separate occasions (Table 2).
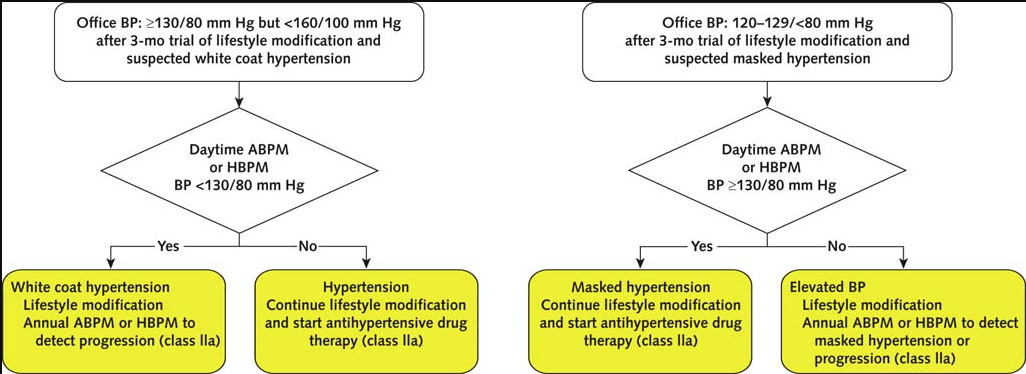
The guideline recommends greater use of out-of-office BP measurements to confirm the diagnosis of hypertension and titrate medication. In adults who are not using antihypertensive drugs, ambulatory BP monitoring (ABPM) or home BP monitoring (HBPM) should be used to detect white coat hypertension (high office BP but normal out-of-office BP) and masked hypertension (normal office BP but high out-of-office BP) (Figure 1). White coat hypertension is associated with a CVD risk approximating that of normal BP, whereas masked hypertension carries a CVD risk similar to that of sustained hypertension. In adults already using antihypertensive drugs, the guideline recommends screening for masked uncontrolled hypertension if the office BP is at goal but CVD risk is increased or target organ damage is present. If the office BP is more than 5 to 10 mm Hg above goal in a patient using 3 or more antihypertensive drugs, the guideline recommends HBPM to detect a white coat effect (Figure 2).
Secondary Hypertension
A secondary cause of hypertension can be identified in approximately 10% of hypertensive adults, and specific treatment of the cause reduces CVD risk. Screening for a secondary cause is recommended in the circumstances listed in Table 3, with referral to a clinician with relevant expertise when screening results are positive.
Nonpharmacologic Interventions
Lifestyle changes alone are recommended for most adults newly classified as having stage 1 hypertension (130 to 139/80 to 89 mm Hg), and lifestyle changes plus drug therapy are recommended for those with existing CVD or increased CVD risk. Recommended lifestyle interventions are listed in Table 4.
BP Goals for Patients With Hypertension
Table 4 summarizes recommendations on BP thresholds and goals for treatment of adults with hypertension. After initiation of antihypertensive drug therapy, regardless of ASCVD risk, the recommended BP target is less than 130/80 mm Hg. The quality of evidence supporting this target is stronger for patients with known CVD or an estimated 10-year ASCVD risk of at least 10% than for patients without elevated risk. A recent systematic review and network meta-analysis showed continuing reduction in CVD risk (major cardiovascular events, stroke, coronary heart disease, and all-cause mortality) at progressively lower levels of achieved SBP (13). A sensitivity analysis demonstrated a similar pattern when the results of SPRINT (Systolic Blood Pressure Intervention Trial) were excluded (13).
Choice of Antihypertensive Drug Therapy
The evidence review conducted to inform the recommendations found some differences but general similarity in the efficacy and safety of drugs traditionally considered first-line agents, underscoring the importance of BP lowering above the choice of drug (7). Recommendations on initial agents are summarized in Table 4. For adults without a compelling indication for use of a specific drug, clinicians should initiate therapy with thiazide diuretics, calcium-channel blockers, angiotensin-converting enzyme inhibitors, or angiotensin-receptor blockers. Thiazide diuretics (especially chlorthalidone) and calcium-channel blockers are the preferred options for first-line therapy in most U.S. adults because of their efficacy. In black patients, including those with DM, thiazide diuretics and calcium-channel blockers are recommended as first-line agents, whereas β-blockers and renin–angiotensin system inhibitors are less effective at lowering BP.
For patients with stage 2 hypertension, initiation of 2 antihypertensive agents from different classes is recommended when the average SBP and DBP are more than 20 and 10 mm Hg above target, respectively. Patients with stage 2 hypertension and an average BP of 160/100 mm Hg or higher should be treated promptly, should be carefully monitored, and should have prompt adjustment of their regimen until control is achieved.
After initiation of drug therapy, management should include monthly evaluation of adherence and therapeutic response until control is achieved. Interventions to promote control, such as HBPM, team-based care, and telehealth, are useful in improving BP control.
BP Thresholds and Goals in Adults With DM
Although the guideline encourages ASCVD risk assessment in all adults with hypertension, including those with DM, clinicians can assume for the sake of convenience that most adults with DM and hypertension have a 10-year ASCVD risk of at least 10%, placing them in a high-risk category that requires initiation of drug therapy at a BP of 130/80 mm Hg or higher. Although the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial did not document a statistically significant reduction in the primary outcome (CVD composite) with intensive versus standard BP lowering, the trial was underpowered to detect a difference between treatment groups, and interpretation of the results was complicated by use of a factorial design (16). SPRINT demonstrated a CVD benefit from intensive treatment to an SBP goal of less than 120 mm Hg but did not include patients with DM (17). Meta-analysis of the SPRINT and ACCORD results suggested that the findings of both trials were consistent (18). A post hoc analysis of SPRINT suggested that patients with prediabetes derived similar benefit compared with normoglycemic patients (19). Thus, the guideline recommends that antihypertensive drug treatment should be initiated at a BP of 130/80 mm Hg or higher in adults with DM, and the treatment goal should be less than 130/80 mm Hg (Table 4).
BP Thresholds and Goals in Adults With CKD
Hypertension has been reported in 67% to 92% of patients with CKD, with increasing prevalence as renal function declines. High BP may occur as a consequence of kidney disease, but even in this context, its presence is likely to lead to an acceleration in further kidney injury. Similar to patients with DM, those with CKD and hypertension are automatically assigned to the high–risk category for ASCVD, with the BP threshold for pharmacologic treatment at 130/80 mm Hg or higher. Given that most patients with CKD die of CVD complications, evidence from SPRINT supports a BP target of less than 130/80 mm Hg for patients with CKD (Table 4) (17).
BP Thresholds and Goals in Older Adults
Hypertension is a leading cause of preventable morbidity and mortality in older adults and is a major contributor to their premature disability and institutionalization. Isolated systolic hypertension is the predominant form of hypertension in older persons. Randomized trials of antihypertensive therapy have included large numbers of older adults, and in every instance, including when the SBP treatment goal was less than 120 mm Hg, more intensive BP-lowering therapy safely reduced risk for CVD events for those older than 65, 75, and 80 years. Both HYVET (Hypertension in the Very Elderly Trial) and SPRINT included older persons who were frail but still living independently in the community, and both found substantial benefit in those who received more intensive BP treatment (17, 20). Blood pressure–lowering therapy is one of a few interventions that has been shown to reduce risk for death in frail older adults. Initiation of BP-lowering therapy, especially with 2 drugs, should be done with caution in older persons, and careful monitoring for adverse effects, including orthostatic hypotension, is essential.
Although the guideline encourages ASCVD risk assessment in all adults with hypertension, including older persons, clinicians can assume for the sake of convenience that adults aged 65 years or older with hypertension have a 10-year ASCVD risk of at least 10%, placing them in a high-risk category that requires initiation of drug therapy at an SBP of 130 mm Hg or higher. Treatment of hypertension with an SBP goal of less than 130 mm Hg is recommended for noninstitutionalized, ambulatory, community-dwelling adults aged 65 years or older with an average SBP of 130 mm Hg or higher (Table 4). Careful titration of BP-lowering medications and close monitoring are especially important in older adults with a high burden of comorbidity because large trials have excluded many such persons. For older adults (aged ≥65 years) with hypertension, a high burden of comorbidity, and limited life expectancy, clinical judgment, patient preference, and a team-based approach to assess the risk–benefit tradeoffs of treatment are reasonable for decisions about the choice of drug and intensity of BP control (Table 4).
Management of Resistant Hypertension
Resistant hypertension is defined as an average office BP of 130/80 mm Hg or higher in patients adhering to 3 or more antihypertensive agents from different classes at optimal doses, including a diuretic, or in those requiring 4 or more antihypertensive medications. Using the former BP target of less than 140/90 mm Hg, the prevalence of resistant hypertension has been estimated to be 13% among hypertensive adults. Estimates suggest that the prevalence of resistant hypertension will be about 4% higher with the new BP target of less than 130/80 mm Hg (4). Risk for myocardial infarction, stroke, end-stage renal disease, and death in adults with resistant hypertension (using the previous definition) is 2- to 6-fold higher than in adults with hypertension that is not resistant to treatment. Clinicians caring for patients who fulfill the criteria for resistant hypertension should ensure that the diagnosis is based on accurate office BP measurements, assess for nonadherence to the prescribed antihypertensive medications, and obtain home or ambulatory BP readings to rule out the white coat effect. Contributing lifestyle factors should be identified and addressed. Use of substances that interfere with antihypertensive therapy, such as nonsteroidal anti-inflammatory drugs, stimulants, and oral contraceptives, should be discontinued or minimized, and secondary causes of hypertension should be excluded.
Treatment of resistant hypertension includes maximization of diuretic therapy (chlorthalidone or indapamide instead of hydrochlorothiazide), addition of a mineralocorticoid receptor antagonist (spironolactone or eplerenone), addition of mineralocorticoid receptor antagonist (spironolactone or eplerenone), addition of other agents with different mechanisms of action, use of loop diuretics in patients with CKD, and referral to a hypertension specialist if BP remains uncontrolled (Table 5).
Strategies to Improve Hypertension Treatment and Control
Every adult with hypertension should have an evidence-based care plan that promotes treatment and self-management goals, effective management of comorbid conditions, timely follow-up, and CVD guideline–directed management (Table 5). Up to 25% of patients do not fill their initial prescription for antihypertensive drug therapy, and only 1 in 5 patients has sufficiently high adherence to achieve the benefits observed in randomized controlled trials (21). Once-daily dosing of antihypertensive medication and use of combination pills can improve adherence.
A team-based care approach is recommended for adults with hypertension. In addition, use of the electronic health record and patient registries is beneficial in recognizing uncontrolled hypertension and guiding initiatives for quality improvement in hypertension control. Telehealth strategies also can be useful adjuncts to interventions shown to lower BP for adults with hypertension.
Summary
Hypertension is a leading risk factor for death and disability-adjusted life-years worldwide. Blood pressure of 120/80 mm Hg or higher is linearly related to risk for fatal and nonfatal stroke, ischemic heart disease, and noncardiac vascular disease, and each increase of 20/10 mm Hg doubles the risk for a fatal CVD event. The 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (4) is the first comprehensive hypertension clinical practice guideline since 2003. The 2017 guideline uses a different classification system for BP than previous guidelines; emphasizes out-of-office BP measurements to confirm the diagnosis of and monitor success in control of hypertension; advocates team-based care and use of the electronic health record and telehealth strategies for improved care; recommends nonpharmacologic interventions; and recommends addition of antihypertensive drug therapy based on a combination of average BP, ASCVD risk, and comorbid conditions.
Appendix: 2017 ACC/AHA Hypertension Guideline Writing Committee
Paul K. Whelton, MB, MD, MPH, Chair*
Robert M. Carey, MD, Vice Chair*
Wilbert S. Aronow, MD†
Donald E. Casey, MD, MPH, MBA†
Karen J. Collins, MBA†
Cheryl Dennison Himmelfarb, RN, PhD†
Sondra M. DePalma, MHS†
Sammuel Gidding, MD†
Kenneth A. Jamerson, MD†
Daniel W. Jones, MD†
Eric J. McLaughlin, PharmD†
Paul Muntner, PhD†
Bruce Ovbiagele, MD, MSc, MAS†
Sidney C. Smith Jr., MD†
Crystal C. Spencer, JD†
Randall S. Stafford, MD, PhD†
Sandra J. Taler, MD†
Randall J. Thomas, MD, MS†
Kim A. Williams Sr., MD†
Jeff D. Williamson, MD, MHS†
Jackson T. Wright, MD, PhD†
* Author.
† Nonauthor contributor.
TABLE 1 – Click to enlarge

TABLE 2 – Click to enlarge

FIGURE 1 – Click to enlarge
{kind=link}

Algorithm for detection of white coat hypertension or masked hypertension in patients not receiving antihypertensive drug therapy.
Colors correspond to class of recommendation in the Appendix Figure. (Reproduced with permission of the American College of Cardiology and the American Heart Association.) ABPM = ambulatory blood pressure monitoring; BP = blood pressure; HBPM = home blood pressure monitoring.
FIGURE 2 – Click to enlarge

Algorithm for detection of white coat effect or masked uncontrolled hypertension in patients receiving drug therapy.
Colors correspond to class of recommendation in the Appendix Figure. (Reproduced with permission of the American College of Cardiology and the American Heart Association.) ABPM = ambulatory blood pressure monitoring; BP = blood pressure; CVD = cardiovascular disease; HBPM = home blood pressure monitoring.
APPENDIX FIGURE – Click to enlarge
{kind=link}

Applying class of recommendation and level of evidence to clinical strategies, interventions, treatments, or diagnostic testing in patient care*.
COR and LOE are determined independently (any COR may be paired with any LOE). A recommendation with LOE C does not imply that the recommendation is weak. Many important clinical questions addressed in guidelines do not lend themselves to clinical trials. Although RCTs are unavailable, there may be a very clear clinical consensus that a particular test or therapy is useful or effective. (Reproduced with permission of the American College of Cardiology and the American Heart Association.) COR = class (strength) of recommendation; EO = expert opinion; LD = limited data; LOE = level (quality) of evidence; NR = nonrandomized; R = randomized; RCT = randomized controlled trial.
* The outcome or result of the intervention should be specified (an improved clinical outcome or increased diagnostic accuracy or incremental prognostic information).
† For comparative-effectiveness recommendations (COR I and IIa; LOE A and B only), studies that support the use of comparator verbs should involve direct comparisons of the treatments or strategies being evaluated.
‡ The method of assessing quality is evolving, including the application of standardized, widely used, and preferably validated evidence grading tools and, for systematic reviews, the incorporation of an Evidence Review Committee.
TABLE 3 – Click to enlarge

TABLE 4– Click to enlarge

FIGURE 3 – Click to enlarge

BP thresholds and recommendations for treatment and follow-up.
Colors correspond to class of recommendation in the Appendix Figure. (Reproduced with permission of the American College of Cardiology and the American Heart Association.) ASCVD = atherosclerotic cardiovascular disease; BP = blood pressure; CVD = cardiovascular disease.
* Using the American College of Cardiology/American Heart Association Pooled Cohort Equations. Patients with diabetes mellitus or chronic kidney disease are automatically placed in the high-risk category. For initiation of use of a renin–angiotensin system inhibitor or diuretic therapy, clinicians should assess blood tests for electrolytes and renal function 2 to 4 wk after initiating therapy.
† Clinicians should consider initiation of pharmacologic therapy for stage 2 hypertension with 2 antihypertensive agents from different classes. Patients with stage 2 hypertension and BP ≥160/100 mm Hg should be promptly treated, carefully monitored, and subject to upward medication dose adjustment as necessary to control BP. Reassessment includes BP measurement, detection of orthostatic hypotension in selected patients (e.g., older patients or those with postural symptoms), identification of white coat hypertension or a white coat effect, documentation of adherence, monitoring of response to therapy, reinforcement of the importance of adherence, reinforcement of the importance of treatment, and assistance with treatment to achieve the BP target.
TABLE 5 – Click to enlarge

References
1. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010., Lancet, 2012, vol. 380 (pg. 2224-60)
2. Forouzanfar MH, Liu P, Roth GA, Ng M, Biryukov S, Marczak L, et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015., JAMA, 2017, vol. 317 (pg. 165-82)
3. Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J, Murray CJ, et al. The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors., PLoS Med, 2009, vol. 6 pg. e1000058
4. Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines., Hypertension, 2017
5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureNational Heart, Lung, and Blood Institute. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure., Hypertension, 2003, vol. 42 (pg. 1206-52)
6. Gibbons GH, Harold JG, Jessup M, Robertson RM, Oetgen WJ. The next steps in developing clinical practice guidelines for prevention., Circulation, 2013, vol. 128 (pg. 1716-7)
7. Reboussin DM, Allen NB, Griswold ME, Guallar E, Hong Y, Lackland DT, et al. Systematic review for the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines., Hypertension, 2017
8. Jacobs AK, Anderson JL, Halperin JL, Anderson JL, Halperin JL, Albert NM, et al. ACC/AHA Task Force Members. The evolution and future of ACC/AHA clinical practice guidelines: a 30-year journey: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines., Circulation, 2014, vol. 130 (pg. 1208-17)
9. Thomopolous C, Parati G, Zanchetti A. Effects of blood pressure lowering on outcome incidence in hypertension: 7. Effects of more vs less intensive blood pressure lowering and different achieved blood pressure levels—updated overview and meta-analysis of randomized trials., J Hypertens, 2016, vol. 34 (pg. 613-22)
10. Xie X, Atkins E, Lv J, Bennett A, Neal B, Ninomiya T, et al. Effects of intensive blood pressure lowering on cardiovascular and renal outcomes: updated systematic review and meta-analysis., Lancet, 2016, vol. 387 (pg. 435-43)
11. Verdecchia P, Angeli F, Gentile G, Reboldi G. More versus less intensive blood pressure-lowering strategy: cumulative evidence and trial sequential analysis., Hypertension, 2016, vol. 68 (pg. 642-53)
12. Bangalore S, Toklu B, Gianos E, Schwartzbard A, Weintraub H, Ogedegbe G, et al. Optimal systolic blood pressure target after SPRINT: insights from a network meta-analysis of randomized trials., Am J Med, 2017, vol. 130 (pg. 707-19)
13. Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, Mills KT, et al. Systolic blood pressure reduction and risk of cardiovascular disease and mortality: a systematic review and network meta-analysis., JAMA Cardiol, 2017, vol. 2 (pg. 775-81)
14. Muntner P, Carey RM, Gidding S, Jones DW, Taler SJ, Wright JT Jr, et al. Potential U.S., population impact of the 2017 American College of Cardiology/American Heart Association high blood pressure guideline, Circulation. 2017
15. Goff DC Jr, Lloyd-Jones DM, Bennett G, Coady S, D’Agostino RB, Gibbons R, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines2013 ACC/AHA guideline on the assessment of cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines., Circulation, 2014, vol. 129 (pg. S49-73)
16. Cushman WC, Evans GW, Byington RP, Goff DC Jr, Grimm RH Jr, Cutler JA, et al. ACCORD Study GroupEffects of intensive blood-pressure control in type 2 diabetes mellitus., N Engl J Med, 2010, vol. 362 (pg. 1575-85)
17. Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. SPRINT Research GroupA randomized trial of intensive versus standard blood-pressure control., N Engl J Med, 2015, vol. 373 (pg. 2103-16)
18. Perkovic V, Rodgers A. Redefining blood-pressure targets—SPRINT starts the marathon [Editorial]., N Engl J Med, 2015, vol. 373 (pg. 2175-8)
19. Bress AP, King JB, Kreider KE, Beddhu S, Simmons DL, Cheung AK, et al. SPRINT Research GroupEffect of intensive versus standard blood pressure treatment according to baseline prediabetes status: a post hoc analysis of a randomized trial., Diabetes Care, 2017
20. Warwick J, Falaschetti E, Rockwood K, Mitnitski A, Thijs L, Beckett N, et al. No evidence that frailty modifies the positive impact of antihypertensive treatment in very elderly people: an investigation of the impact of frailty upon treatment effect in the HYpertension in the Very Elderly Trial (HYVET) study, a double-blind, placebo-controlled study of antihypertensives in people with hypertension aged 80 and over., BMC Med, 2015, vol. 13 pg. 78
21. Berra E, Azizi M, Capron A, Høieggen A, Rabbia F, Kjeldsen SE, et al. Evaluation of adherence should become an integral part of assessment of patients with apparently treatment-resistant hypertension., Hypertension, 2016, vol. 68 (pg. 297-306)